담관암 (cholangiocarcinoma, CCA)
위험인자: 담관 점막의 만성적 자극, 담즙 저류
choledochal cyst, sclerosing cholangitis, clonorchiasis, chronic supprative cholangitis, alcoholic liver disease, gallstone(choledocholithiasis)
분류
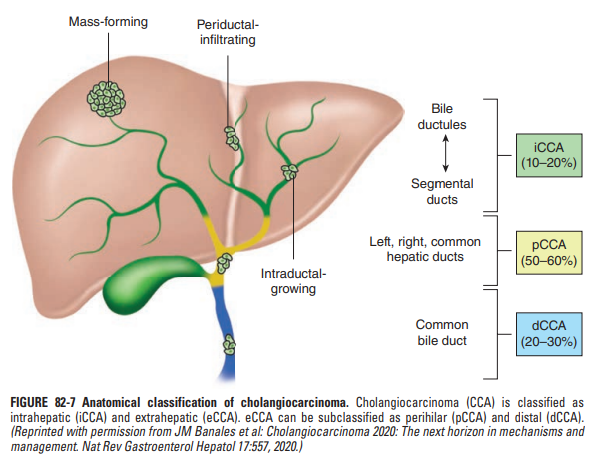
간내 담관암 (intrahepatic cholangiocarcinoma)
간외 담관암 (extrahepatic cholangiocarcinoma)
간문부 담관암(=perihilar cholangiocarcinoma = hilar cholangiocarcinoma = Klatskin tumor): cystic duct 합류부위 보다 상방인 경우
원위부 담관암 (distal cholangiocarcinoma): cystic duct 합류부위 보다 하방인 경우
증상 : 무통성 황달, 가려움증, 체중감소 등
Courvoisier’s sign : painless palpable RUQ mass
(중하부 CBD에 발생한 암에 의해 확장된 쓸개가 통증 없이 촉지되는 소견)
검사 : 빌리루빈, ALP, CA19-9 상승
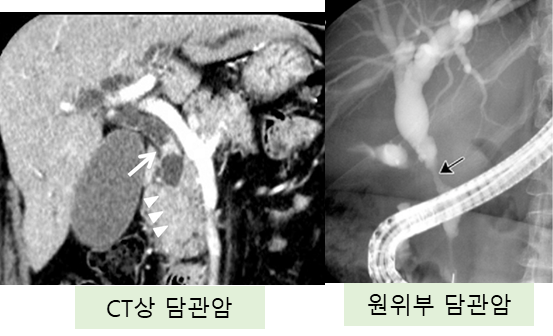
영상 : 초음파, 복부 CT or MRI, ERCP, PTC (percutaneous transhepatic cholangiography)
→ 영상 소견 상 담관암은 대부분 mass forming type, periductal infiltrating type, intraductal growing type 중 하나를 보이게 됨
치료 : 침범 범위에 따라 치료법이 상이, 수술적 절제가 근본적인 치료. 절제 불가능한 경우 고식적 치료 및 항암치료 시행
[1] Harrison 21e, pg.653-656
[2] Sabiston 21e, pg.1519-1525
간내담관암 (iCCA)
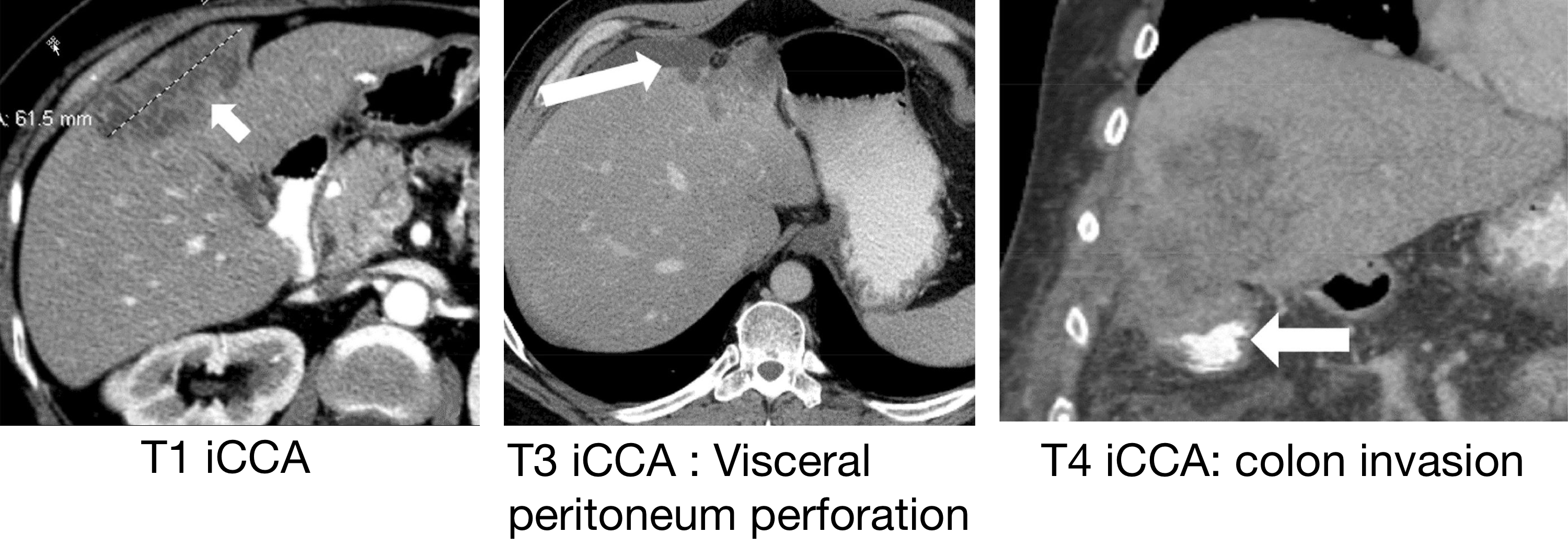
Single tumor (T1) / multinodular tumor or vascular invasion (T2) : 절제가능
Resection 후 보조항암요법 (capecitabine)
Visceral peritoneum perforation (T3) / direct invasion of extrahepatic structures(T4) / N1 / M1 : 절제 불가능
간내병변만 존재하는 경우 → TACE/TARE 또는 전신 항암화학요법 (gemcitabine + cisplatin)
간외병변도 존재 → 전신 항암화학요법
[1] Harrison 21e, pg.653-656
간문부담관암 (pCCA)
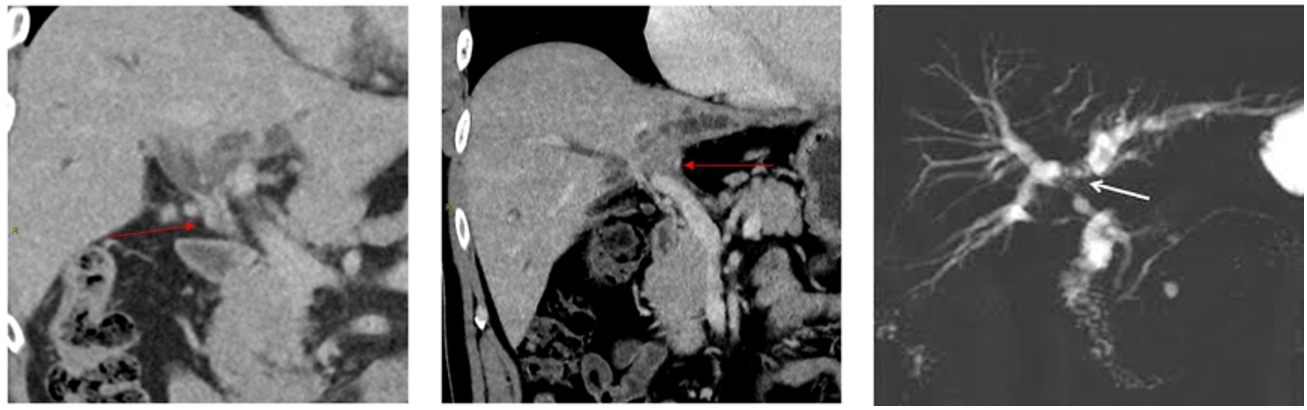
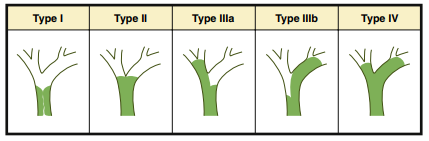
modified Bismuth-Corlette 분류: 좌우 hepatic duct 의 침윤 범위를 기술하는 분류
type I: tumor involving only the common hepatic duct below hilar confluence
type II: tumor involving the hilar confluence without involvement of the secondary ductal confluences
type IIIA: tumor involving the right secondary ductal confluence
type IIIB: tumor involving the left secondary ductal confluence
type IV: tumor involving both the right and left secondary ductal confluence
치료: 수술적 절제 → 항암화학요법
Type 1,2: 침범된 담관 절제 + 쓸개절제 + 간 국소절제 (2는 caudate lobe도 절제)
Type 3: 침범된 담관 절제 + 쓸개절제 + Rt(3a) or Lt(3b) hepatectomy + Caudate lobe 절제
Type 4: 과거에는 수술 불가능한 경우로 여겨졌으나, 최근에는 절제가능한 경우라면 extensive resection 을 시도하는 추세
절제불가: 항암화학요법 (Gemcitabine + cisplatin ± pembrolizumab/durvalumab), 고식적 치료 (스텐트 담즙 배액, 통증 조절 등)
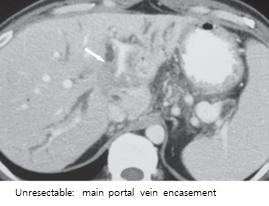
절제불가 담관암의 기준
Extensive disease extending to bilateral secondary biliary confluences without favorable anatomy/anatomical variants
Vascular involvement of the HA or PV without possibility of reconstruction
(tumor involvement more than 50% of the vessel circumference)Inadequate volume of FLR due to atrophy or deep parenchymal invasion
Distant nodal or visceral metastases
[1] Sabiston 21e, pg.1519-1525
[2] Preoperative Imaging Assessment and Staging of Perihilar Cholangiocarcinoma: Tips and Pitfalls, J Korean Soc Radiol. 2025 Jan;86(1):45-67
[3] Radiologic Evaluation and Structured Reporting Form for Extrahepatic Bile Duct Cancer: 2019 Consensus Recommendations from the Korean Society of Abdominal Radiology, Korean J Radiol 2021;22(1):41-62
원위부 담관암 (dCCA)
치료
절제 가능: 췌십이지장절제술 (PPPD or Whipple 수술)
절제 불가능: 항암화학요법, 고식적 완화 치료 (gemcitabine + cisplatin ± prembrolizumab/durvalumab)
간외담관암의 담즙 배액
절제가능한 간외담관암의 수술 전 담관배액술 (preoperative biliary drainage for resectable extrahepatic CCA)
과거에는 폐쇄성 황달이 있는 환자에서 수술 전 담즙배액술을 시행하여 황달을 개선하면 수술 예후가 좋아질 것이라는 기대가 있었으나, 최근 연구들에서는 불필요한 배액술이 오히려 합병증을 증가시킬 수 있음이 밝혀졌다. 따라서 수술 전 담즙 배액은 모든 환자에게 routine하게 시행하지 않고, 특정한 경우에 이득을 고려하여 시행하게 된다.
적응증
담관 폐쇄로 인한 담관염, 패혈증등의 합병증이 발생한 경우
bilirubin >10 mg/dL 이상의 폐쇄성 황달을 보이는 경우
간절제 후 잔존 간 부피 (FLR) <30-50% 가 예상되는 경우
방법: ENBD, ERBD, PTBD 등 폐쇄 위치 및 환자 협조 가능성 등을 고려하여 선택
절제불가능한 간외담관암의 담관 배액술 (palliative bile drainage for unresectable extrahepatic CCA)
간문부 담관암: proximal 한 병변일수록 경피적 배액술 (PTBD)이 내시경 접근보다 더 일반적으로 더 유용 (bismuth type I-II에서는 ERCP가 선호되며, type III-IV에서는 PTC가 더 효과적)
원위부 담관암: 금속 스텐트를 이용한 내시경 담관 배액술(ERCP, ENBD)을 우선 고려
(환자가 불안정하거나 협조가 어려운 경우, 과거 수술이나 해부학적 변이로 내시경을 십이지장까지 삽입하기 어려운경우, 담관암이 국소적으로 진행된 경우 등에서는 PTBD 선호)
이미 위축된 부위에는 스텐트 배액을 시행하지 않음
[1] Sabiston 21e, pg.1520,1524
[2] Extrahepatic cholangiocarcinoma: Current status of endoscopic approach and additional therapies, World J Hepatol. 2021 Feb 27;13(2):166–186
[3] 2023 간외담관암 진료 가이드
[4] 2025 NCCN Extrahepatic Cholangiocarcinoma
0개의 글
** 제목만 보더라도 어떤 내용인지 알 수 있도록 완성된 문장으로 작성해주세요.
예시) 초음파 (X) → 초음파 사진에서 PDA 소견을 어떻게 알 수 있나요? (O)